Best Practices for Effective Strategy Execution
Effective strategy execution is crucial for success, as even the most well-crafted strategies can fail if not properly implemented.

Effective strategy execution is crucial for success, as even the most well-crafted strategies can fail if not properly implemented.

Five-year strategic plans in home care often encounter several challenges due to the dynamic nature of the industry.

Adaptive leadership is not a fixed set of rules or practices; rather, it's a mindset and a skill set that empowers leaders to thrive in turbulent times.

CMS is asking for feedback to create a future episode-based payment model seeking feedback regarding a potential new episode-based payment model that would be designed with a goal to improve beneficiary care and lower Medicare expenditures by reducing fragmentation and increasing care coordination across health care settings.

Fostering effective team-based care improves both the patient’s and the team’s experience of care delivery. In this article, we discuss the two different approaches to team-based care, the five core principles, and how to reduce clinician burnout.

July/August 2024 Issue
FREE CONTENT In this issue of The Remington Report, we cover many aspects of social determinants of health. Get valuable insights, trends, and tools your organization can utilize to build referral partners, support patients and their families, and improve outcomes.

July/August 2024 Issue
SUBSCRIBER CONTENT Universal Foundation Measures is a framework designed to foster a collaborative approach to quality reporting and improvement across healthcare settings and payers. This initiative aims to promote unity among all healthcare providers, emphasizing the collective effort in shaping the future of quality measures.

July/August 2024 Issue
SUBSCRIBER CONTENT Hospitals are using required screening tools to identify the risk factors of social determinants. Results will expand referral relationships to improve meaningful collaboration between healthcare providers and community-based organizations. Get to know the key reasons this is important to your organization.

July/August 2024 Issue
SUBSCRIBER CONTENT Obtain Z codes prior to a patient's discharge to gather crucial information that can assist your organization in identifying non-medical conditions and social and economic factors. We will guide you on how to locate them.

July/August 2024 Issue
SUBSCRIBER CONTENT A groundbreaking consumer survey has unveiled key insights into how your organizations can enhance their social determinants of health. Your understanding of these top preferences can revolutionize your approach, underscoring the importance of your role in this process.

July/August 2024 Issue
SUBSCRIBER CONTENT Medicaid MCOs, as key players in the healthcare system, are increasingly focused on social determinants of health. They are implementing strategies to reduce these determinants and improve patient outcomes. Get the current trends and learn what’s ahead, so you can better collaborate with these organizations and enhance patient outcomes.

July/August 2024 Issue
SUBSCRIBER CONTENT Noora Health’s Health Companion Program enhances family and caregiver knowledge, boosts professional development for aides, and gives your organization a competitive edge. Discover the key insights of this innovative program.

One-third of all fee-for-service Medicare beneficiaries receiving post-acute care have a diagnosis of dementia, and more than 7 in 10 receive this care in a SNF.

According to the Bureau of Labor Statistics, overall employment of nurse practitioners is projected to grow 45% by 2030.

In this article is the legal case between referrals: assisted living, independent living facilities, and home health, details of the ruling, and what to consider in a referral relationship agreement.

May/June 2024 Issue
FREE CONTENT The home care industry lies at the center of chronic care management. It holds the key to reducing the overall cost of care, minimizing readmissions, emergency department visits, and offering value propositions that align with partnerships involving hospitals, health systems, ACOs, payers, and Medicare Advantage Plans.

May/June 2024 Issue
SUBSCRIBER CONTENT Are you aware that both Medicare and Medicare Advantage beneficiaries are eligible for the Chronic Care Management program? It presents a remarkable opportunity to offer comprehensive care to those grappling with multiple chronic conditions. However, despite the widespread prevalence of chronic illnesses among Medicare beneficiaries, only a fraction is using the program. Which physicians are leveraging the program most frequently? What are the challenges?

May/June 2024 Issue
SUBSCRIBER CONTENT It's often assumed that heart disease ranks highest for medical condition expenditure in home healthcare. Get ready to be surprised by the real leader in medical expenditure.

May/June 2024 Issue
SUBSCRIBER CONTENT Unlocking insights that profile frequent emergency department visits and common chronic conditions unveils the critical medical conditions linked to your patient management.

May/June 2024 Issue
SUBSCRIBER CONTENT Personal care private duty agencies, it's crucial to recognize that fraud and abuse enforcement aren't exclusive to services covered by the Medicare Program. In fiscal year 2023 alone, there were 279 criminal convictions associated with private duty home care services. It's vital to understand the implications.
May/June 2024 Issue
SUBSCRIBER CONTENT In 2024, approximately 2.4 million individuals with Alzheimer’s dementia are aged 85 or above. Research indicates that patients who receive home health services following hospital discharge have a higher chance of staying in their community for at least 30 days post-discharge, with more significant advantages observed with extended durations of home health care.

May/June 2024 Issue
SUBSCRIBER CONTENT Unlocking business insights into the total cost of care for patients with chronic conditions, with and without home care personal services, presents compelling findings that strengthen value propositions to your referrals.

May/June 2024 Issue
SUBSCRIBER CONTENT CMS has unveiled the Direct Care Workforce Strategies Center, a pivotal initiative aimed at tackling the pressing shortage of workers providing direct care to elderly and disabled individuals. Worker registries play a crucial role in addressing fundamental questions: Who meets the criteria to deliver Home and Community-Based Services in each state, and how can Medicaid beneficiaries connect with them?

Care Continuum: Reports just published prove ACOs are saving Medicare money! The next generation ACO is expanding and testing home care through six new benefits including waivers, expanding the role of the nurse practitioner and piloting a value-based payment. This went into motion July 1. We explain in detail how this impacts home care.

Readmission after skilled-nursing facility (SNF) discharge following heart failure hospitalization is highest during the first two days home.

The emergency department (ED) is the hospital's front door, providing over 70% of all hospital admissions. How can home-based care providers partner with EDs?

March/April 2024 Issue
FREE CONTENT The surge in collaborations between home care providers and referral sources is creating fresh avenues for growth and fostering opportunities for deeper relationship-building. Fostering relationships involves cultivating meaningful connections and collaboration. The increase in referral partnerships between home care and referral partners can be attributed to seven key factors.

March/April 2024 Issue
SUBSCRIBER CONTENT ACO MarketScan: What makes it crucial for home care providers to establish connections with ACOs? With more than half of Medicare beneficiaries enrolled in accountable care organizations, aiming for 100%, home care providers must craft compelling value propositions and engagement strategies to foster partnerships.

March/April 2024 Issue
SUBSCRIBER CONTENT Hospital MarketScan: A thorough grasp of hospital quality and outcomes proves highly advantageous for home care providers. Establishing and fortifying referral partnerships with hospitals and health systems necessitates a more comprehensive understanding of hospital outcomes and quality measures to enhance relationship building efforts.

March/April 2024 Issue
SUBSCRIBER CONTENT Physician MarketScan: As CMS concentrates on integrating more specialists into value-based care, prioritizing engagement with home care providers emerges as a key strategic imperative. These engagement strategies center around areas such as readmissions, care transitions, longitudinal care, value-based payments, bundled payments, and the expansion of specialty care within a home setting.

March/April 2024 Issue
SUBSCRIBER CONTENT Case managers or discharge planners found in violation of the anti-kickback statute may face criminal prosecution, potentially leading to prison sentences and other repercussions. If you were aware or should have been aware, you may bear responsibility. Attorney Elizabeth Hogue provides detailed explanations of these implications.

March/April 2024 Issue
SUBSCRIBER CONTENT One specific area of concern is transportation, given its high priority. Missed medical appointments incur costs of up to $150 billion annually for the healthcare industry. What is your organization's strategy to address this challenge?

March/April 2024 Issue
SUBSCRIBER CONTENT Patients possess the right to select their care
providers, and this choice is reinforced through various avenues embedded in policies and regulations. Attorney Elizabeth Hogue explains the key touchpoints.

March/April 2024 Issue
SUBSCRIBER CONTENT Hospital at home updates you may have missed.

The top five conditions most used for hospice.

Discharge planners, case managers, and social workers certainly cannot accept cash payments from providers in exchange for referrals of patients. But what can they accept from providers who want referrals?

Getting to know the nursing workforce by state helps to know states with the most job openings, salaries, and the best and worst states to work. We give you the intel.

January/February 2024 Issue
FREE CONTENT In the January/February issue of The Remington Report, we answer two critical questions. What are the most critical areas of change in 2024? How can your organization better anticipate the future, identify opportunities, and confidently grow? Our four environmental scans will get you ready for 2024.

January/February 2024 Issue
SUBSCRIBER CONTENT ENVIRONMENTAL SCAN: Payments are shifting the site of care, accelerating the growth of care at home. The movement of ortho and cardiac payments from impatient to outpatient is related to increased volumes of care in the home. We provide forecasts and the impact to home care organizations.

January/February 2024 Issue
SUBSCRIBER CONTENT ENVIRONMENTAL SCAN: Team-based and multidisciplinary teams underpin the success of value-based care models and hospitals-at-home. Cross-collaborative teams in specialty clinical programs are making their way between hospitals and home care organizations. This is the next level of clinical integration and for stakeholders to better understand home care’s value.

January/February 2024 Issue
SUBSCRIBER CONTENT ENVIRONMENTAL SCAN: Referrals are more dependent on home care as partners for financial, quality, and patient experience measures. Shifting payments are changing traditional views of managing a patient’s care journey. Each segment of healthcare will contribute to a synergistic success level. No organization can do it alone.

January/February 2024 Issue
SUBSCRIBER CONTENT ENVIRONMENTAL SCAN: Screening requirements for social determinants in 2024 are front and center for hospitals, dialysis centers, physicians, and post-acute providers. Coordination across various healthcare settings, including ambulatory, emergency department, inpatient, and home health will create a unified approach.

January/February 2024 Issue
SUBSCRIBER CONTENT The Department of Health and Human Services encourages stakeholders across the health continuum to formalize Community Care Hubs to manage social determinants of health. We explain the meaning behind Community Care Hubs and conceptual models.

January/February 2024 Issue
SUBSCRIBER CONTENT The issues impacting prior authorizations from managed care organizations have caused some providers to discontinue relationships with plans. Starting January 1, 2024, UnitedHealthcare is changing home health agency processes.

January/February 2024 Issue
SUBSCRIBER CONTENT The value-based insurance design model will be required to address health-related social needs in at least two of three health-related social needs areas: food, transportation, and housing insecurity and/or living environment, and improve care coordination. Get the changes affecting hospice and the list of 2024 participants.

This report finds the most recent shifts in senior’s social determinants of health, urgent needs to support older Americans, long-term trends, and the health of older Americans.

November/December 2023 Issue
SUBSCRIBER CONTENT It has become a national priority to understand the needs of high-need, high-cost patients. In this article, we hear the voices of patients and how to prevent ED visits and readmissions.

November/December 2023 Issue
SUBSCRIBER CONTENT More hospitals will face readmissions penalties in 2024, per preliminary CMS data. The Centers for Medicare and Medicaid Services will restart its pneumonia readmissions measure.

November/December 2023 Issue
SUBSCRIBER CONTENT According to a recent analysis of Bureau of Labor Statistics data, home healthcare is one of the most dangerous places to work in healthcare. Homecare field staff members who provide services on behalf of private duty agencies, hospices, Medicare-certified home health agencies, and home medical equipment companies are extremely vulnerable.

November/December 2023 Issue
SUBSCRIBER CONTENT A coaching framework of techniques and tools employed by health providers is part of an intensive care management intervention and an Authentic Healing Relationship between patients and care teams.

November/December 2023 Issue
SUBSCRIBER CONTENT A respected biennial health insurance survey sheds light on the burden seniors face to afford medications and care that are enrolled in traditional Medicare and Medicare Advantage plans.

November/December 2023 Issue
SUBSCRIBER CONTENT Coaching interventions have been widely touted as a potential way to prevent chronic illness and to help patients better self-manage their chronic illnesses. Coaching draws from a range of strategies to tailor its response to the dynamic situation of patients and their families.

November/December 2023 Issue
SUBSCRIBER CONTENT New York State’s new requirement for certain certificate-of-need applications includes a health equity impact assessment. New York is now the first state to implement a required equity assessment in its health facility planning and approval process that went into effect June 22.

Research shows that social determinants can be more important than health care or lifestyle choices in influencing health. Numerous studies suggest that SDOH account for between 30-55% of health outcomes.

According to the Bureau of Labor Statistics, registered nursing is one of the fastest-growing occupational fields in the country.

This study provides insight into the long-term care services and support needs of seniors that help shape the future.

The focus on social determinants of health in 2023 is uniting payers and providers to increase their efforts to find solutions and improve outcomes. Driven by policy and payments, change is coming.

September/October 2023 Issue
SUBSCRIBER CONTENT On June 6, 2023, CMS issued a that when a patient is discharged from a hospital, it is important to provide post-acute providers and caregivers as applicable with the appropriate patient information related to a patient’s treatment and condition to decrease the risk of readmission or an adverse event.

September/October 2023 Issue
SUBSCRIBER CONTENT A Judge issued an opinion and order, in which he said that the State of Florida must provide services, including private duty nursing care, to medically fragile children who are living in nursing homes or threatened with institutionalization so that they can live at home.

September/October 2023 Issue
SUBSCRIBER CONTENT For CY 2024, CMS proposes paying physicians for Caregiving Training Services (CTS) when the treating practitioner identifies a need to involve and train one or more caregivers to assist the patient in carrying out a patient-centered treatment plan.

September/October 2023 Issue
SUBSCRIBER CONTENT The study is based on eight focus groups that included nurses, physicians, discharge planning staff, and patients. It identified areas of possible change to the discharge planning process to reduce instances of unplanned hospital readmissions.

September/October 2023 Issue
SUBSCRIBER CONTENT CMS is proposing to pay separately for Community Health Integration, Social Determinants of Health (SDOH) Risk Assessment, and Principal Illness Navigation services to account for resources when clinicians involve community health workers, care navigators, and peer support specialists in furnishing medically necessary care.

September/October 2023 Issue
SUBSCRIBER CONTENT The eight-year Guiding an Improved Dementia Experience Model (GUIDE) seeks to keep Medicare enrollees outside of long-term care facilities by extending a package of local care coordination and management and caregiver education and support services.

July/August 2023 Issue
SUBSCRIBER CONTENT This article identifies four essential attributes of the growth in Medicare Advantage Plans and interesting other facts.

July/August 2023 Issue
SUBSCRIBER CONTENT Three new and proposed policies and regulations are reshaping critical areas of healthcare, including social determinants of health, Medicare, Medicaid, and Medicaid Managed Care. Taking a deeper look helps to predict future changes.

July/August 2023 Issue
SUBSCRIBER CONTENT A new CMS model for primary care is testing value-based payments, chronic care management, and management of social determinants. If successful, the model Making Care Primary can scale both large and small physician practices into value-based care and comprehensive care management.
July/August 2023 Issue
SUBSCRIBER CONTENT A ruling from the Supreme Court may make it more difficult for enforcers to prove liability under the False Claims Act and more manageable for providers to defend themselves against claims of violations.

July/August 2023 Issue
SUBSCRIBER CONTENT The HCBS workforce is not growing fast enough to serve residents relying on long-term services and support. New investments in this workforce are essential to sustain access to HCBS for current and future generations.

July/August 2023 Issue
SUBSCRIBER CONTENT Some telehealth waivers extended under COVID reached their end, while others continue through December 31, 2024. This article provides an easy way to know the current status of telehealth waivers in each health care sector.

July/August 2023 Issue
SUBSCRIBER CONTENT The paradox is 85% of patients in the US prefer to die at home, but only 40% die at home or in hospice. A recent study examined the association between the presence of state palliative legislation and the place of death.

May/June 2023 Issue
SUBSCRIBER CONTENT Disruptors or non-traditional providers are quickly accelerating their footprint into the care-at-home market. These providers are addressing the pain points and healthcare gaps that traditional-for-service providers have failed to correct for many years.
May/June 2023 Issue
FREE CONTENT Learn the five key areas that home-based care organizations could assist in discharge planning.

May/June 2023 Issue
SUBSCRIBER CONTENT Learn the results of a homecare agency’s audit and appeals case.
May/June 2023 Issue
SUBSCRIBER CONTENT Learn the perspectives of patients regarding their care transition experience after discharge.

May/June 2023 Issue
SUBSCRIBER CONTENT The Expanding Care in the Home Act: By moving an array of services for Medicare beneficiaries from hospital to home, lawmakers hope they can save money while allowing older Americans to receive care in their homes. Get an understanding of a new proposed bill.

May/June 2023 Issue
FREE CONTENT In this special report, we provide guidance to help your organization improve the clinician experience and gather data to easily track satisfaction and achieve a more engaged workforce.

March/April 2023 Issue
SUBSCRIBER CONTENT The importance of key ACO trends is to better understand the plan to decrease fee-for-service and increase value-based payments. Growth through three initiatives will be the foundation to reach CMS’s goal of 100% of Medicare into an accountable care program.

March/April 2023 Issue
SUBSCRIBER CONTENT Learn the seven reasons why ACOs use home care and what’s behind the motivation.

March/April 2023 Issue
SUBSCRIBER CONTENT Preferred-provider agreements are an important strategy for increasing referral relationships. This article provides a greater understanding of the legal aspects.

March/April 2023 Issue
SUBSCRIBER CONTENT This article summarizes the major provisions of the new ACO Reach Model and the expanded role of home-based care providers.

March/April 2023 Issue
SUBSCRIBER CONTENT The profile of seniors is changing according to the Administration on Aging. Get the latest information.

March/April 2023 Issue
SUBSCRIBER CONTENT A study out of the Ohio State University Fisher College of Business explores factors that can help ACOs deliver more efficient and effective health care, by how much and the costs associated with these improvements.

March/April 2023 Issue
SUBSCRIBER CONTENT Compliance with HIPAA can be complex. Examples of violations, or “HIPAA stories,” may make requirements more understandable. We share some of those stories.

The model aims to improve the overall health of Marylanders, reduce avoidable hospital readmissions and emergency department visits, and improve the patient experience in health care settings.

A 1995 court decision involving Caremark established that members of boards of directors likely have liability for non-compliance with fraud and abuse prohibitions. A recent Court decision likely extends liability to individual corporate officers.

To identify efficient HHAs, CMS examined cost efficiency and quality at freestanding HHAs to identify a cohort that demonstrated better performance on these metrics relative to peers.

Nearly 60 percent of Medicare hospice spending in 2020 was for patients with stays exceeding 180 days.

Hospice quick fact market overview from the latest data.

Compliance with HIPAA can be complex. Examples of violations, or “HIPAA stories,” may make requirements more understandable. Here are some of those stories.

January/February 2023 Issue
SUBSCRIBER CONTENT Key studies and data can help providers reduce readmissions, improve outcomes, and increase partnerships.

January/February 2023 Issue
SUBSCRIBER CONTENT New social determinants of health (SDOH) quality measures will be required by hospitals, health plans, and multi-payer federal and state programs. We provide details on how each healthcare sector will be incorporating SDOH quality measures.

January/February 2023 Issue
SUBSCRIBER CONTENT Home care is big business for payers. No better industry is more aligned with payer goals than home-based care. We address six strategies to evaluate contracting with Medicare Advantage plans.

January/February 2023 Issue
SUBSCRIBER CONTENT Medicare’s Care Compare website is adding physician and clinician affiliations to home-based care organizations. The new information is meant to provide additional information to support patients and caregivers as they make healthcare decisions.

January/February 2023 Issue
SUBSCRIBER CONTENT In this article, we explore the models of care advancing health equity and the closer connection to value-based care.

January/February 2023 Issue
SUBSCRIBER CONTENT The Medicare Payment Advisory Commission submitted its official payment recommendations to Congress for March FY2024. Recommended cuts include home healthcare and hospice.

January/February 2023 Issue
SUBSCRIBER CONTENT Medicaid-funded personal care services and home healthcare services will need to be fully compliant with their state’s electronic visit verification systems by January 1, 2023. We review the oversight and details.
January/February 2023 Issue
SUBSCRIBER CONTENT CMS has indicated that the agency intends for anyone with Medicare coverage to be under a value-based payment arrangement by 2030. Learn which fee-for-service programs are advancing value-based care.

As a home-based care provider, all referral partners have the same goal – how to reduce readmissions and the cost. It’s important to continue to hone in on data that can help your organization better understand your role in preventing readmissions and reducing the cost of care.

New information will help your organization better align clinical services to reduce the cost of the highest medical conditions and their expenditures. The data can be used in conversations with various payer sources to align your organization’s services to reduce the cost of care and readmissions.
November-December 2022 Issue
SUBSCRIBER CONTENT Care transitions promote improved outcomes when discharge planning, home-based care, physicians, and hospitalists engage on the first day of an inpatient admission.

November-December 2022 Issue
SUBSCRIBER CONTENT Home-based organizations eager to have partnerships with ACOs will learn in our discussion why certain ACOs engage in greater home visits and care transitions to manage complex patients. No two ACOs are alike. Get insights into the characteristics of ACOs and their decision points. We follow up with three key leadership discussion questions.
November-December 2022 Issue
SUBSCRIBER CONTENT The focus on social determinants of health is a hot topic in healthcare. Multidisciplinary teams and a care transition model in the case study resulted in reduced readmissions and improved outcomes. The model is scalable and a win-win for healthcare and the patient.

November-December 2022 Issue
FREE CONTENT In this special report, we provide 36 ways your investment in technology can produce a positive ROI across your organization. We identify the right technologies to get a positive return on your investment.

November-December 2022 Issue
SUBSCRIBER CONTENT Sharp HealthCare pre-hospice program called Transitions, is designed to give elderly patients the care they want at home and keep them out of the hospital.

November-December 2022 Issue
FREE CONTENT In our extensive resource of special reports, you’ll find actionable solutions to improving care transitions, real-time communications with team members, and what patients want for better communications. These complimentary resources offer solutions to workforce shortages, clinician burnout, and advancing solutions in home-based care.

November-December 2022 Issue
SUBSCRIBER CONTENT Seven areas of healthcare are changing in 2023 related to quality measures, bundled payments, the hospice benefit, and the expanded HHVBP model. For each, we provide details and resources to keep you in the know.

“Poaching agreements” may produce artificial suppression of employees’ compensation and may violate the federal Sherman Act.

The Office of Inspector General has stated that there are two major types of fraud and abuse compliance that must be addressed through ongoing evaluation processes.

Practitioners owe a duty of care in the diagnosis and treatment of patients even though they are working under the supervision of licensed physicians.

The crisis level of the nursing shortage has no easy fix. A national survey provides insights into what are the most important benefits for nurses, how salaries compare nationwide, and what are the most crucial factors for job satisfaction.

September/October 2022 Issue
SUBSCRIBER CONTENT With all the evolving changes occurring in healthcare, you may have missed CMS’s initiatives aligning value-based arrangements across traditional Medicare programs. We discuss the eight trends to help your organization think about the impact on your labor force and referral partners.

September/October 2022 Issue
SPECIAL REPORT In this special report, we provide 11 strategic actions to improve your care team's productivity both internally and externally. Get insights into advancing clinical communications with your referral partners, ways your care team always has real-time patient status, and how to improve the referral process. Don't miss the eight additional resources to dig even deeper into this topic.

September/October 2022 Issue
SUBSCRIBER CONTENT The role of the nurse practitioner continues to grow with more than 355,000 NPs nationwide and growth projections of 45% by 2030. We provide important state-by-state analysis and annual salaries.

September/October 2022 Issue
SPECIAL REPORT/FREE CONTENT In this special report, learn about the challenges and solutions to effective care transitions, competitive tools, and shared peer actions.

September/October 2022 Issue
SUBSCRIBER CONTENT The gap between the younger generation and the senior population is narrowing when it comes to smart phones, tablets, internet users, YouTube, and telehealth. A recent study provides valuable insight for healthcare providers adopting technology in the home.

September/October 2022 Issue
SUBSCRIBER CONTENT $60 million in investments will expand and improve the rural community workforce. We provide details and resources for each.

September/October 2022 Issue
SPECIAL REPORT What are the four questions leadership should explore to optimize scheduling with continuity of care and staff utilization? In this special report, we answer these four questions and give you solutions to help provide better care to more patients, while making the most of your staff’s time. This effort starts with their scheduling process.
September/October 2022 Issue
SUBSCRIBER CONTENT The job outlook for home health and personal care aides is growing much faster than all occupations. Our analysis breaks it down by state and wages.

According to the most recent MedPAC report, the number of home health agencies has been declining since 2013 after several years of substantial growth.
Payers are developing care models specific to the level of need. There is not a one-size-fits-all care-management strategy. Payers tend to categorize medical conditions by risk.

Case managers/discharge planners continue to come under fire from fraud enforcers for violations of the federal anti-kickback statute.

July/August 2022 Issue
SUBSCRIBER CONTENT How should your organization be responding to payers expanding their position in home-based care? What key trends support this advancement? What are key strategies to partner and align with payers? In this article, we cover the key market changes, the disruption, and growth opportunities for home-based care organizations.
July/August 2022 Issue
SUBSCRIBER CONTENT Payers are deepening their care delivery models focused on the home. In the past, we may have thought of payers in traditional roles as a medical-cost manager. Today, they are acquiring home-based care organizations to control readmissions, cost, and outcomes.

July/August 2022 Issue
SUBSCRIBER CONTENT Different payers such as Medicare, Medicare Advantage, and Special Needs Plans are focusing on the highest chronic care conditions to reduce the cost of care. In this article, is the data by payer and a discussion about how organizations can support a better aligned financial and quality partnerships.

July/August 2022 Issue
SUBSCRIBER CONTENT Medicare Advantage enrollment is growing at a fast pace. The number of plans is expanding geographically, and payers will continue to invest in the Medicare Advantage market. In this article, we dig deep into the growth of Medicare Advantage by enrollment, states, and the future. The market signal is strong to put Medicare Advantage contracting as a high priority.

July/August 2022 Issue
SUBSCRIBER CONTENT Important to all payers is the value your organization brings to reducing the cost of care. Available data can gear-up your partnership value quickly. In this article, we sliced and diced data to provide an overall macro/micro picture of how to reduce the cost of care.

July/August 2022 Issue
SPECIAL REPORT/FREE CONTENT What do family caregivers identify as important areas for choosing care-at-home provider? What area did family caregivers identify for improvement? How are your organization’s surveys being affected? What strategies made the top of the list? What are the five ways to achieve family caregiver communication success? In this special report, we give you seven family caregiver expectations to increase your competitive advantage.

A recent study in the Journal of Managed Care was an eye-opener when it comes to better understanding home-based care from an ACO perspective.

It’s a new environment for anti-trust enforcement, especially in the healthcare industry. Providers should pay close attention to this issue.

Increase your partnership value with hospitals by leveraging this study, which showed home health vs. no post-acute care was associated with reduced 30-day readmissions and better outcomes.

Patients discharged with heart failure from a skilled-nursing facility to home face the highest risk of readmissions in the first two days after a SNF discharge.

Achieving a timely transition of care while simultaneously lowering the risk of readmission remains one of the toughest challenges in the quest for value-based outcomes.

May/June 2022 Issue
SUBSCRIBER CONTENT Hospitals are responsible for coding a Medicare beneficiary discharge bill based on the discharge plan for the patient. Here's what you need to know.

May/June 2022 Issue
FREE CONTENT The discharge status code identifies where the patient is being discharged to at the end of their facility stay or transferred to such as an acute/post-acute facility.

May/June 2022 Issue
SUBSCRIBER CONTENT A recent study published in the American Journal of Managed Care showed home health vs. no post-acute care was associated with reduced 30-day readmissions and better outcomes.

May/June 2022 Issue
SUBSCRIBER CONTENT Medicare’s IPPS post-acute care transfer policy requires hospitals to apply the correct discharge status code to claims where patients receive home health services within three days of discharge.

May/June 2022 Issue
SUBSCRIBER CONTENT This important OIG report has finding of hospitals that did not properly code post-acute transfer correctly.

May/June 2022 Issue
SUBSCRIBER CONTENT Fast facts about the Post-Acute Transfer Policy. Here's what you need to know at a glance.

May/June 2022 Issue
SUBSCRIBER CONTENT Medicare improperly paid acute-care hospitals $54.4 million for 18,647 claims subject to the Post-Acute Care Transfer policy.

A recent study published in the Journal of the American Medical Association of 5,464 beneficiaries reveals that total health expenditures were lower for those who used hospice.
To prove that providers rendered negligent wound care, patients must prove all of the following: Duty, breach, cause, and injury or damage.

Analysis of trends and payment patterns indicate non-hospice payments for Medicare Part A and B items and services totaled $6.6 billion from 2010 through 2019.

Although the trend is certainly against non-compete agreements or restrictive covenants in the health care industry, some state courts have affirmed their use.

March/April 2022 Issue
SUBSCRIBER CONTENT Discharge destinations require established relationships with a network of high-quality post-acute providers, facilities and home health resources in the community.

March/April 2022 Issue
FREE CONTENT Data Sharing: Number of readmissions, readmission rates, and average cost of readmissions

March/April 2022 Issue
SUBSCRIBER CONTENT Researchers examined the common reasons why some hospitals have more readmissions treating a disproportionate share of patients with low incomes, poor health and other negative circumstances.

March/April 2022 Issue
SUBSCRIBER CONTENT The federal government’s effort to penalize hospitals for excessive patient readmissions is ending its first decade with Medicare cutting payments to nearly half the nation’s hospitals.

March/April 2022 Issue
FREE CONTENT Percentage of Medicare aged 66-74 enrolled in Medicare fee-for-service within 30-days of hospital discharge.

March/April 2022 Issue
SUBSCRIBER CONTENT A recent analysis determined that Medicare fee-for-service patients who received personal care services experienced a decrease in Medicare expenditures over time.

March/April 2022 Issue
FREE CONTENT A recent study examined the patterns of Medicare beneficiaries post-acute care transitions among assisted living residents and their outcomes in the first 30 and 60 days after hospital discharge.

January/February 2022 Issue
SUBSCRIBER CONTENT CMS’s reinterpretation of “primarily health-related” benefits has led to more Medicare Advantage (MA) plans offering services.

January/February 2022 Issue
SUBSCRIBER CONTENT CMS projects that nearly 30 million people are signing up for MA in 2022. Here are seven trends to watch for.

January/February 2022 Issue
SUBSCRIBER CONTENT CMS is testing a broad array of complementary MA health plan innovations designed to reduce Medicare program expenditures, enhance the quality of care for Medicare beneficiaries

January/February 2022 Issue
FREE SPECIAL REPORT Seven trends supporting growth and the future, including the expansion of community-based care and expanded clinical care models to attract referrals.

January/February 2022 Issue
SUBSCRIBER CONTENT Z codes are a set of ICD-10-CM codes used to report social, economic, and environmental determinants known to affect health and health-related outcomes.

January/February 2022 Issue
FREE CONTENT Case managers/discharge planners continue to come under fire from fraud enforcers for violations of the federal anti-kickback statute.

January/February 2022 Issue
SUBSCRIBER CONTENT According to the U.S. Bureau of Labor Statistics' latest occupational employment and wage statistics survey, the mean annual wage for nurse practitioners in the U.S. is $114,510.

January/February 2022 Issue
SUBSCRIBER CONTENT The median annual wage for home health and personal care aides was $27,080 in May 2020, according to the U.S. Bureau of Labor Statistics.

The owner of a supplier of home medical equipment (HME) complained that her company did not receive referrals from TidalHealth Nanticoke Hospital. The Court dismissed the owner’s lawsuit because she could not prove her claims. This case illustrates why providers who complain about practices of referral sources must have facts to support their claims.

Launched in 2018, Huntsman at Home in Utah was one of the first programs in the United States to provide acute cancer care at home.

In a November 2021 decision, the U,S, Court of Appeals said that CMS can recoup overpayments from providers even though its appeals are still pending before Administrative Law Judges.

Providers, including marketers, are tempted to give patients free items and services. But be careful! These activities may violate laws prohibiting providers that participate in state and federal health programs from giving free items and services to patients.

November-December 2021 Issue
SUBSCRIBER CONTENT Medicare Advantage beneficiaries are switching to Medicare Fee-for-Service during their last year of life, according to a Government Accountability Office report.

November-December 2021 Issue
FREE CONTENT Interviews with two organizations share how they tackled challenges to improve medical supply management, reduce the cost of care, and improve outcomes.

November-December 2021 Issue
SUBSCRIBER CONTENT Learn the association between the timing of home healthcare start of care and 30-day rehospitalization outcomes for Medicare beneficiaries following a diabetes-related hospitalization.

November-December 2021 Issue
SUBSCRIBER CONTENT Four peers share solutions to improve clinical handoffs, the advantages of timely information, how to drive better outcomes, and how to boost clinical productivity.

November-December 2021 Issue
SUBSCRIBER CONTENT Get insight into how ACOs are performing and related changes to their future.
November-December 2021 Issue
SUBSCRIBER CONTENT This study provides insight into the long-term care services and support needs of seniors that help shape the future.

SUBSCRIBER CONTENT Across the board, we see from referral sources and other care providers alike that they really feel as if they’re part of the care team now instead of the end of the line where a patient goes when they get out of the hospital. Your peers share their thoughts and solutions.

November-December 2021 Issue
FREE CONTENT Effective on January 19, 2021, new regulations related to the Stark laws expanded and underscored the ability of hospitals to require physicians to send referrals to particular providers. These new regulations also make it clear that providers can monitor and enforce requirements to direct referrals to designated providers.
SPECIAL REPORT Interviews with two organizations share how they tackled challenges to improve medical supply management, reduce the cost of care, and improve outcomes.

Your partners – ACOs, payers, commercial insurers, physicians, and health systems – seek ways to reduce hospitalizations and re-hospitalizations. A critical measurement of your value is to show how your organization can reduce the cost of care, decrease re-hospitalizations, and improve outcomes.

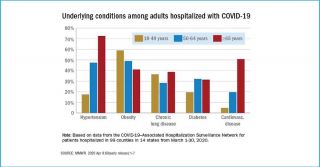
The 18th annual report by Trust for America’s Health on the obesity crisis in the United States has been released. This year, special features highlight the interaction of the COVID-19 pandemic with social, economic, and environmental conditions that impact hospitalizations, social determinants of health (SDOH), and outcomes.

September/October 2021 Issue
FREE CONTENT In this article, we discuss the 10 most frequent principal diagnoses and their costs impacting hospital inpatient stays.

September/October 2021 Issue
SUBSCRIBER CONTENT Learn the specific six surging areas businesses are investing in that is creating a road map to healthcare’s future.

September/October 2021 Issue
SUBSCRIBER CONTENT Your referral partners increasingly expect robust communications to make patient transfers as seamless as possible, for both the patient and providers. They will have to make a choice. Ultimately, they will look for relationships with organizations that are easy to work with and that can deliver proven quality care. We provide insights and strategies from high-performing organizations.

September/October 2021 Issue
SUBSCRIBER CONTENT Read the insights about home-based primary care and how they have reduced hospitalizations, readmissions, and emergency room visits.
September/October 2021 Issue
SUBSCRIBER CONTENT The American Hospital Association is urging CMS to keep five COVID waivers and to not return to the old ways of doing things.

September/October 2021 Issue
SUBSCRIBER CONTENT Recent research discusses the missed opportunities for discussions about end-of-life, including advance care planning, palliative care, discontinuation of disease-directed treatment, hospice care, and after-death wishes, with outpatients with advanced cancer.

September/October 2021 Issue
SUBSCRIBER CONTENT In this new normal, it’s important to understand how your referral sources work, what they are sending to you versus the competition, how to deepen relationships with these sources, and what differentiates you as a provider in the marketplace.
SPECIAL REPORT Your referral partners increasingly expect robust communications to make patient transfers as seamless as possible, for both the patient and providers, which means you need strategies to create seamless transitions. Learn what leading home health and hospice agencies are doing in this free special report.

July/August 2021 Issue
SUBSCRIBER CONTENT Four significant trends are impacting chronic care management and the future of physician groups and payers. Moving forward this can change your referral growth and the need to expand your managed care contracts.

July/August 2021 Issue
SUBSCRIBER CONTENT Payers are targeting their member populations that will benefit the most from at-home care. The center of their home health offerings is focused on high-cost patients, palliative care, diabetes, home care visits, telehealth, and at-home testing.

July/August 2021 Issue
SUBSCRIBER CONTENT A recent study found receiving certain forms of care at home instead of in the hospital can lower healthcare spending. Administering specialty drugs at home or in a provider’s office lowered healthcare spending by $4 billion.

July/August 2021 Issue
SUBSCRIBER CONTENT Strategies and actions to improve clinician experiences. Work/life balance is something nurses are constantly trying to achieve, and many nurses are falling short of that goal. What solutions are your peers using to combat burnout, achieve better nurse work/life balance, and improve patient care?

July/August 2021 Issue
FREE CONTENT In this article, we take a look at social determinant insights and investments from the perspective of Medicare Advantage plans, Medicaid managed care and healthcare providers.

July/August 2021 Issue
SUBSCRIBER CONTENT Primary care transformation in voluntary programs has failed to broadly engage primary care organizations. What’s causing the low participation?

July/August 2021 Issue
SUBSCRIBER CONTENT How to empower your team, drive efficiency of care, prevent readmissions, and gain a competitive advantage for your home health and/or hospice agency.

The Remington Report presents six ways to accelerate home health and hospice growth through improved referral processes, including questions you should be asking your referral sources.

A new report from the GAO titled, "COVID-19 Program Flexibilities and Considerations for Their Continuation," investigates the future of telehealth

SPECIAL REPORT Work-life balance is something nurses are constantly trying to achieve, and many nurses are falling short of that goal. Here, then, are strategies and actions to improve clinician experiences.

What are the fraud implications when patients' rights are violated? What is the role of physicians in patients' freedom of choice? The Remington Report gets answers from Attorney Elizabeth Hogue.

SPECIAL REPORT How to empower your team, drive efficiency of care, prevent readmissions, and gain a competitive advantage for your home health and/or hospice agency.

May/June 2021 Issue
Payers, health systems, Private Equity firms, and SPAC’s acquisition of care at home companies are quickly changing market dynamics, and signaling change is ahead. This is a must-read to understand trends and insights reshaping the future.

May/June 2021 Issue
Your referral sources are the lifeblood of your organization. Ultimately, they will look for relationships with organizations that are easy to work with and that can deliver proven quality care. A new research report reveals the four frustrations felt by your referral sources. A roundtable of your peers' weigh-in with solutions.

May/June 2021 Issue
The National Institute of Health advance care planning studies are focusing on the effectiveness of telehealth for patients receiving home-based palliative care and leveraging in home support services to engage patients in advance care planning. Learn more about the pilot studies supporting this research.

May/June 2021 Issue
The right of patients to choose providers has generated considerable conflict within the provider community. In this article, learn the four key legal sources supporting patient choice and actions your organizations and patients can take to have them enforced.

May/June 2021 Issue
A review of payment models under CMS’ Center for Medicare and Medicaid Innovation (CMMI) is quietly under review to decide if they will be implemented. Many of these models were popular with care at home providers. We provide insight into each of these payment models.

May/June 2021 Issue
The Remington Report interviews Nick Knowlton to discuss how to manage referrals, grow referrals, exchange communications with referrals, and gain a competitive advantage.

SPECIAL REPORT What referring hospitals, ACOs, and physicians want from home health, hospice, palliative care and private duty providers to make their lives easier.

SPECIAL REPORT For five top strategies, we discuss actionable steps that can be taken by home health, hospice, palliative care, and private duty organizations to gain a competitive advantage.

Educational materials, tools, training, and resources for integrating palliative care into ambulatory care for patients with serious life-threatening chronic illness or conditions.

March/April 2021 Issue
Expanding continuum of care services is an important strategy for future market positioning. We explore how providers, payers, and physicians are broadening services to expand partnership referrals, create innovation, and ensure sustainability.
March/April 2021 Issue
New information will help your organization better align clinical services to reduce the cost of the highest medical conditions and their expenditures. The data can be used in conversations with various payer sources to align your organization’s services to reduce the cost of care and readmissions.

March/April 2021 Issue
Under Andrew Molosky’s leadership, Chapters Health System has combined innovation and creative disruption to shift end-of-life care into a leading community-based population health organization.

March/April 2021 Issue
Post-acute organizations need consulting physicians’ services. The OIG continues to scrutinize these relationships. What are the three things providers should know before signing agreements?

March/April 2021 Issue
National leaders discuss how to lean into new approaches to accelerate growth, improve performance, and address technologies that create faster reimbursement, better work-life balance for clinicians, and optimal patient outcomes.

SPECIAL REPORT The compelling ways business intelligence drives actionable results.

SPECIAL REPORT National leaders discuss how to lean into new approaches to accelerate business growth, improve performance, and address technologies that create faster reimbursement, better work-life balance for clinicians, and optimal patient outcomes. They share how their organizations address four key questions.
On a temporary basis, CMS issued blanket Section 1135 to healthcare professionals in response to the COVID-19 public health emergency (PHE). But now the OIG wants to be sure the rules are being followed. This Remington Report special report dives into the subject of home health telehealth payments.
SPECIAL REPORT The shift from end-of-life care to building a continuum-based approach, plus strategies for growth, market position, and innovation revealed.
This year, several value-based payment models will begin the shift from fee for service to value-based. Earmark this as the transformation of payment reform for care-at-home providers and how they will be paid in the future. This white paper explains the seven value-based models impacting care-at-home providers.

January/February 2021 Issue
Beginning in 2021, several value-based payment models will begin the shift from fee-for-service to value-based. Earmark this as the transformation of payment reform for care at home providers and how they will be paid in the future.

January/February 2021 Issue
New choices to receive care at home centers on patients receiving acute level care in the home. Non-traditional care at home models is expanding into a new era. The twist to non-traditional programs is to keep care at home leadership’s eyes wide open about the impact to their organizations. Waivers are changing rules, policies have changed, and the role of who can care for patients in the home is transforming models.

January/February 2021 Issue
The invisible technology boundaries expand the rules of who can offer care in the home, how they will be paid, and it creates a less restrictive policy environment to deliver care at home. The opportunity to reshape care delivery and create a more efficient and cost-effective healthcare system is achievable because of the acceleration and adoption of technology.

January/February 2021 Issue
The question for leadership is how do you want to position your organization? As an integrator? Or as an aggregator? For care at home providers, the goal is to create a post-acute continuum model as patients transition from one care setting to another whether that be in-home personal care services, skilled home health, palliative care, or hospice.

January/February 2021 Issue
Geographic direct-contracting model (GEO) is the latest CMS Center for Medicare and Medicaid Innovation (CMMI) model which allows Direct Contracting Entities to accept full financial risk for all traditional Medicare enrollees in their region. Three options enhance Medicare benefits and provide waivers for care in the home.

January/February 2021 Issue
A growing number of initiatives are expanding to address social determinants of health. Payers, health systems, community-based organizations, and government entities are partnering together to create statewide efforts to improve community health and social care.

January/February 2021 Issue
Medicare Advantage growth continues to outpace overall Medicare FFS membership growth, according to the latest statistics.

January/February 2021 Issue
Why should we be concerned that primary care spending appears to be declining? A growing body of evidence measuring health system performance and population health outcomes finds that greater primary care is associated with better value: enhanced population health outcomes, greater equity, and more efficient use of healthcare resources.

Your organization has new opportunities to grow and expand payer partnerships. A one-size-fits-all approach no longer exists, which is why we have bundled four articles from the Nov-Dec 2020 issue of The Remington Report into this complimentary compendium. Read about how to expand internal and external education, leverage critical investments in your workforce, and enhance actionable data needed by payers.
Home-based medical care models are shaking-up the $260 billion primary care market. Three physician models, new reimbursement models, telehealth, and chronic care management are key drivers.
In this free industry report, The Remington Report provides key data analysis to help your organization mitigate COVID-19 readmissions, along with five action steps for your organizations to explore.

November-December 2020 Issue
Home-based medical care models are shaking-up the $260 billion primary care market. Three physician models, new reimbursement models, telehealth, and chronic care management are key drivers.

November-December 2020 Issue
Building home care capacity will give plans more flexibility to meet patients on their own terms and could improve outcomes. Learn what is changing models of care in the home.

November-December 2020 Issue
States are developing plans to increase Medicaid provider participation in and adoption of value-based care models. How will these new payment models work?

November-December 2020 Issue
Medicare Advantage Plans are expanding supplemental benefits in 2021. Learn what services are expanding and how this expands your partnerships.

November-December 2020 Issue
States are expanding value-based payments (VBP) in Medicaid and leveraging their Medicaid managed care programs to advance their payment reform goals. We discuss the details.

November-December 2020 Issue
CMS' innovation center (CMMI) is about to roll out a new model allowing insurance plans to take on financial risk for patients enrolled in both Medicare and Medicaid. How will this affect payers? What other new models can you expect in the future?

November-December 2020 Issue
The Community Health Access and Rural Transformation (CHART) Model expands telehealth services, links residents to non-local healthcare providers, and provides more than $8.7 million in grant funding. What are the new opportunities for your organization?
November-December 2020 Issue
Compelling stories from your peers talk about their experiences with COVID-19 and their patients.

November-December 2020 Issue
We share a collection of stories from caregivers on the frontline overseeing patient care for multiple conditions at home: dementia, end-of-life, behavioral health, and falls.

November-December 2020 Issue
This collection of stories shares how caregivers overcome the challenges of treating patients during COVID-19.

November-December 2020 Issue
In Advisory Opinion No. 18-05; issued on June 18, 2018; the OIG addressed the circumstances under which providers can establish “caregiver centers” that provide or arrange for free or reduced-cost support services to caregivers in local communities.
In this free industry report, The Remington Report shares six ways care in the home is changing the future of healthcare. Leaders will need to address these strategically if they intend to realize continued growth in a significantly changing marketplace.
In this free industry report, The Remington Report unveils the major reason why patients are not getting home health care after a hospital discharge referral, plus four strategies you can use to boost referrals.
In this free industry report, The Remington Report offers up four strategies to increase the utilization of home health and hospice in the age of COVID-19.

September/October 2020 Issue
Primary care is being rapidly redefined today right before our eyes. As healthcare evolves, patient needs expand and providers must look for new and better ways to achieve a patient-centered model of practice. Read the four reasons home-based primary care is opening doors and opportunities for patients and providers today.

September/October 2020 Issue
How is COVID-19 delaying care? Nationwide 40% of Americans are still delaying care according to a survey from the U.S. Census Bureau.

September/October 2020 Issue
CMS has released proposed policy changes for 2021 Medicare payment rates under its annual Physician Fee Schedule. Telehealth codes allow physicians to bill for home visits and care planning. We dive into the codes and what they mean.

September/October 2020 Issue
Home-based medical care models are shaking-up the $260 billion primary care market. How are integrated primary care delivery models addressing chronic care management in the home?

September/October 2020 Issue
Insurers' strategies to provide greater services in the home are moving rapidly. Changing models have insurers partnering-up with primary care physicians, telehealth, and pharmacies to deliver care in the home. We provide insights to insurers' reactions post COVID-19 and beyond.
September/October 2020 Issue
Payers are interested in talking about the data. In particular, they are interested in understanding how home care providers are able to reduce their penalties and increase their rewards in a value-based payment system. Learn how one organization is advancing conversations.
September/October 2020 Issue
How do anti-kickback statutes apply if providers or Assisted Living Facilities (ALFs) are involved in referral arrangements and receive any type of federal or state funds? Attorney Elizabeth Hogue breaks it all down.

In this article, we take a look at data reflecting the costliest medical conditions by payers. This becomes an important strategy as payers begin to move more value-based care contracting into the home care space and look to treating higher acuity patients in the home.

CMS released a data snapshot of COVID-19 hospitalizations, length of stay, and discharge status for 109,607 patients. Payer sources include Fee-for-service (FFS) claims data, Medicare Advantage (MA) encounter data, and Medicare enrollment information.

Wound care is a risky business these days. Providers who render wound care services are at risk for many things, including liability for negligent wound care, violation of fraud and abuse prohibitions based on substandard wound care, and liability for abandonment when wound care services are discontinued.

CMS has made three new appointments to their quality division, the Visiting Nurse Service of New York has settled its lawsuit, and Orlando Health and LHC Group has inked a partnership. The latest executive moves in healthcare, along with other industry business news, can be found here.

July/August 2020 Issue
Telehealth is healthcare’s hottest topic. How should providers support and drive growth? What new opportunities will improve outcomes? How will telehealth reshape care delivery?

July/August 2020 Issue
Medicare Advantage penetration continued to grow following the 2020 Medicare Annual Election Period, reaching 36.0% in 2020, according to CMS’s March data release.
July/August 2020 Issue
How can home care optimize telehealth during COVID-19 to work with other stakeholders and maintain continuity of care? What strategies can increase uptake and new models?

July/August 2020 Issue
Intermountain at Home’s hospital-level care in patient’s homes supports their health system in the event of a surge of COVID-19 patients. Their models include home-based post-hospital care, palliative, and end-of-life care as well as medical equipment maintenance.

July/August 2020 Issue
CMS has provided blanket waivers with a retroactive effective date of March 1, 2020 through the end of the emergency declaration to help providers during COVID-19. We gathered the waivers for discharge planning, in-home care providers, and other post-acute care settings.
July/August 2020 Issue
The hospitalization rate for COVID-19 is 4.6 per 100,000 population, and almost 90% of hospitalized patients have some type of underlying condition, according to the Centers for Disease Control and Prevention (CDC).

July/August 2020 Issue
CommonSpirit Health at Home provides another layer of protection and defense to keep vulnerable patients safe, healthy, and in their homes during this pandemic. And, it positioned to play a key role in preventing a post-COVID surge at care sites. Learn how CommonSpirit at Home expanded its virtual monitoring capabilities to better respond to patients’ needs during and beyond the COVID-19 pandemic.

July/August 2020 Issue
The reauthorization of the Older Americans Act (OAA) was perfect timing when COVID-19 reared its ugly head. Last March, President Trump signed a bipartisan reauthorization of a landmark law that provides more money for programs that help millions of older Americans age in their homes and communities through services including Meals on Wheels, family caregiver support, and transportation.

July/August 2020 Issue
Amid COVID-19 pandemic, 91% of Medicare Advantage beneficiaries using telehealth report favorable experiences while a record-setting 99% express satisfaction with their MA plan. 78% are willing to use it again.

The Centers for Medicare and Medicaid Services (CMS) has issued a number of waivers of various requirements for healthcare providers related to discharge planning for hospitals and critical access hospitals (CAHs).

In 2020, Medicare Advantage (MA) plans have doubled the number of condition-specific supplemental benefits from approximately 820 to 1,850. However, the new Special Supplemental Benefits for the Chronically Ill (SBBCI) for 2020 didn’t fare as well.

Twenty-one states have taken action to suspend or waive certain practice requirements for physician assistants in response to COVID-19.

A recent survey across the U.S revealed the devastation of reduced revenue, patient’s refusal to accept physician-ordered care, and loss of the workforce.

3.5 million low-wage workers are in the health and social services industry, with the greatest number of those (1.3 million) working as aides or personal care workers

The data from the Bureau of Labor Statistics found dentists' offices had the most losses with 503,000. Physicians' offices lost 243,000.

May/June 2020 Issue
In our interview with Paula Thompson, RN, MS, CRNI, President and CEO of Fidelity Health Care, we learn how her organization has advanced partnerships with five health systems and physician practices.

May/June 2020 Issue
Anxiety levels are high right now. The COVID-19 outbreak has overtaken our lives, affecting everyone, but especially our patients and families. We no longer have the comfort of a normal routine, and there is no end in sight from this unprecedented pandemic.

May/June 2020 Issue
Is COVID-19 identifying a major gap in DME services? As hospitals discharge patients into their homes or other residential settings to free-up resources and hospital beds, the resultant strain on the provision of DME items and services, particularly for suppliers of home oxygen and ventilators, will significantly increase. Read about unintended consequences.

May/June 2020 Issue
COVID-19 quickly identifies gaps in the health care delivery system. In the acute care hospital, the Respiratory Therapists (RT) is a well-respected team leader in respiratory care. Yet as soon as that patient is discharged, they suddenly lose that supportive RT expertise.

May/June 2020 Issue
It’s an important time to review legal questions and issues related to COVID-19. There is a lot of mis-information flying around and it’s easy for providers to get tripped up. But providers must ensure that they are doing it right in order to avoid a day of legal reckoning that could threaten their businesses in the future.

May/June 2020 Issue
MaineHealth Care at Home began using telehealth in 2001. In our Interview with Donna DeBlois, RN, BSW, MSB, MBA, AHCA, President of MaineHealth Care at Home, we learn how her organization is expanding telehealth to a broader patient population under COVID-19.

Are health care systems, patients, and families prepared for tough conversations and decisions about health care preferences and medical interventions?
Concern for healthcare workers in every setting knows no bounds! Providers' imperative is clear: everything possible must be done to keep them safe.
COVID-19 training and prevention resources at your fingertips. You will find these resources important for compliance and infection prevention.

In its March 2020 report to the Congress, MedPAC makes payment policy recommendations for provider sectors in fee-for-service (FFS).

The Bipartisan Act (BBA) of 2018 Act updated the hospital transfer policy for early discharges to hospice care. The law required that, beginning in FY 2019, discharges to hospice care would qualify as a post-acute care transfer and be subject to payment adjustments.

Aggressive moves by payers teaming up with big players such as CVS are advancing their healthcare programs into the home. How does this impact healthcare organizations?

Landmark estimates about 20 percent of chronically ill patients currently experience a gap in the care they are receiving, which can be addressed through medical care, support and education provided in the home.

The Center for Medicare and Medicaid Innovation’s Emergency Triage, Treat, and Transport (ET3) Model is designed to test expanded care destination alternatives to the ED for Medicare beneficiaries who call 911.

A recent study in the Annals of Internal Medicine found that at-home patients fared better than those in the hospital when it came to price and outcomes.

CMS recently announced the Emergency Triage, Treat, and Transport model, which provides greater flexibility to ambulance care teams to address emergency health care needs of certain Medicare beneficiaries following a 911 call.

How can providers offer support for caregivers? A key way for providers to assist may be to collaborate with charitable organizations in the community.

Encompass Health, in collaboration with McKesson, saved 17% to 19% on their supply spend, increased efficiencies, and achieved greater patient satisfaction.

Medicare Advantage and Part D programs for contract years 2021 and 2022 has provisions changing care management requirements for special needs plans.

Post-acute providers, patients, and their families have very successfully raised issues with hospital administrations related to patients' right to choose.

Nearly 100 U.S. lawmakers submitted a letter to CMS concerned about proposed cuts in Medicare payments for physical and occupational therapy services.

In a proposed rule issued on February 5, CMS announced that beneficiaries with ESRD will be able to enroll in Medicare Advantage Plans starting in 2021.

CMS issued a proposed rule and the Advance Notice Part II to further strengthen and modernize the Medicare Advantage and Part D prescription drug programs.

Physicians are thinking more seriously about how to succeed in the MIPS Cost category. Consider these 5 ways to help physicians reduce costs in healthcare.

CMS is planning to combine and standardize eight separate Compare websites into one point of entry, offer Medicare beneficiaries a consistent look and feel.

Recent federal cases make it quite clear that marketers for home health companies and discharge planners/case managers must just say, "NO!" The "jig is up."

The number of ACOs taking on risk for cost increases grew from 93 ACOs at the start of 2019 to 192 at the start of 2020.

The Medicare Payment Advisory Commission recommended that Congress reduce the payments for Home Health by 7% in 2021.

Kaiser Permanente’s virtual cardiac rehabilitation program has enrolled more than 2,300 patients, making it one of the largest such programs in the U.S.

For the first time since the early 20th century, the home has become the common place among American’s dying of natural causes.

Post-acute ACO adds 200 new long-term care facilities, new appointments, home medical equipment acquisitions, mergers and acquisitions, and more.

An integrated program of services can contribute to reducing the cost of care and services to Medicare beneficiaries residing in seniors housing.

Now is the time for all home care providers to review agreements and their practices with regard to payments to referring physicians.
The tides are shifting the expectations of home care. Pressure from reimbursement, shifting payment models, and value-based care are driving the change.

Physical therapists once in such high-demand are facing massive layoffs across the industry because of reimbursement changes to skilled nursing facilities .

CMS is increasing payment for transitional care management services provided after discharge from an inpatient stay or certain outpatient stays.

Starting November 1, UnitedHealthcare will not pay for unplanned surgeries in an outpatient setting unless it determines the site is medically necessary.

What post-acute care providers need to know about a new rule that includes updated payment policies, payment rates, and quality provisions for services furnished under the Medicare Physician Fee Schedule.

The new rules will give providers in value-based arrangements greater certainty and ease the compliance burden for providers across the industry.

The proposed rules recognize that incentives are different in a healthcare system that pays for value rather than the volume of services provided.

Falls were the leading reason for readmission among patients whose initial hospital was fall-related and who were discharged to home, even with home care.
Falls were the leading reason for readmission among patients whose initial hospital was fall-related and who were discharged to home, even with home care.

Private Medicare plans will soon include expanded plan options for seniors, more telehealth, and innovative plan designs and payment models.

Including unpaid caregivers into discharge planning for the elderly patient population reduces readmissions.

New Discharge Planning Conditions of Participation require hospitals to assist patients, their families/caregivers in selecting a post-acute care provider.

Medicare Advantage (MA) Plans are adding two new dementia codes in their risk adjustment payment system and expanding flexibility in the MA benefit design.

A unified value-based incentive program for SNFs, home health services, inpatient rehabilitation facilities, and long-term care hospitals is recommended.

A GAO report explored the efforts to manage high-expenditure beneficiaries, which are 5% of all Medicaid beneficiaries but nearly half of all expenditures.
A unified value-based incentive program for SNFs, home health services, inpatient rehabilitation facilities, and long-term care hospitals is recommended.

Seven guided questions for strategic planning. Six external trends for home care companies to keep an eye on. 10 challenges ahead for home care companies.

Through initiatives that change how heathcare is delivered and physicians are paid, CMS is driving toward the goals of improving quality and reducing costs.

MACRA is a law that builds a new, fast-speed highway to take the healthcare system away from fee-for-service and toward coordinated care models.

CMS published a rule on Merit-Based Incentive Payment System (MIPS) and Advanced Alternative Payment Models (APM) incentives under MACRA.

CMS released the first major regulation under MACRA. For now, only physician offices – not hospitals – are governed by MACRA rules.

Physician and post-acute providers can partner together to provide chronic care management through annual wellness programs visits.

House calls markedly improve the quality of life of home-limited patients and their caregivers while dramatically reducing healthcare costs.

The top six types of providers who provided home-based medical care (non-podiatry) in both 2012 and 2013 accounted for two-thirds of the providers.

Payers and providers are redefining and rethinking how new models of care can move the needle toward value-based care.

Community paramedicine is a new model of healthcare in which paramedics function outside their customary emergency response and transport roles.

A study in the Annals of Emergency Medicine, looked at why heart failure patients go to the Emergency Room.
Including unpaid caregivers into discharge planning for the elderly patient population reduces readmissions.

Study estimates a total annual value opportunity of $31 billion in the Medicare market through integration of mental health medical treatments.
This document answers frequently asked questions about billing chronic care management (CCM) services to the Physician Fee Schedule.

The Stark Law is a set of U.S. federal laws that prohibit physician self-referral, specifically a referral by a physician of a Medicare or Medicaid patient.

Congressional approval of the IMPACT Act in October 2014, mandates the development and implementation of a standardized post-acute care assessment tool.

Section 2(a) of the 2014 IMPACT Act requires post-acute providers to submit standardized patient assessment data, as well as standardized quality measures.

Four healthcare settings must report standardized data using the assessment instruments on at least five of the following eight quality measure domains.

Under the proposed rule, hospitals and critical access hospitals would be required to develop a discharge plan within 24 hours of admission or registration.

n keeping with the requirements of the IMPACT Act, measures for the other domains will be addressed through future rulemaking.

CMS has contracted with Abt Associates and RTI International to develop a cross-setting Post-Acute Care measure for medication reconciliation.

The PPS prototype that has been developed accurately predicts resource needs for nearly all patient groups, indicating it can be used to set fair payments.

CMS issued new guidance to clarify where Medicaid beneficiaries can receive home- and community-based services as defined in a 2014 regulation.

SUBSCRIBER CONTENT Kaiser Permanente Colorado and VNA-Denver jointly offer intense, consistent education to elderly heart failure patients discharged from the hospital.

SUBSCRIBER CONTENT Fragmentation of the care delivery system is widely recognized as a cause of missed opportunities to treat both acute and chronic conditions.

SUBSCRIBER CONTENT The program at Washington Hospital Center has lowered total costs of care and has reduced average inpatient length of stay from 8 to 6 days.

In the proposed rules announced by CMS, SNFs will get an $800 million, or 2.1%, Medicare payment increase under the proposed rule for FY 2017.

SUBSCRIBER CONTENT Key takeaways from the perspective of primary care office help stakeholders to better understand care management population health models.

People who are continuously enrolled in Medicare Advantage are less likely to die in a hospital than those continuously enrolled in Medicare fee-for-service.

All Medicare-certified home health agencies in nine states will compete on value in the HHVBP model, where payment is tied to quality performance.

SUBSCRIBER CONTENT A recent filing by Humana indicates the insurer is instituting a new bonus plan that is not just tied to financial performance, but also to health outcomes.

CPC+ is a national advanced primary care medical home model that aims to strengthen primary care through a regionally-based multi-payer payment reform.

Successful care coordination programs employ a variety of tools to improve quality of care and reduce costs, including flexibility in design.

SUBSCRIBER CONTENT Located in the Bronx and Hudson Valley, New York, Montefiore Health System (MHS) serves one of the poorest and most disproportionately disease-burdened counties in the nation with nearly 80% of the payer mix from Medicare and Medicaid.

In 2011, two-thirds of beneficiaries had three or more chronic conditions, more than one quarter of all beneficiaries reported being in fair or poor health.

CMS recently proposed a new payment model that would bundle payment to acute care hospitals for heart attack and cardiac bypass surgery services.

Care management is a key component of policy development, future legislation and new regulations. How is this changing the future of healthcare?

The OIG held a roundtable to discuss a broad range of ideas regarding how healthcare organizations can measure their compliance program effectiveness.

Cancer accounts for less than one-half of all hospice admissions. Here is a list of the top 13 diagnoses for admissions to hospice care.

SUBSCRIBER CONTENT Multidisciplinary teams across the care continuum work each day to determine the best ways to identify the highest risk patients.

Barriers to palliative care access in the United States occurs in five domains. Learn what these domains are in this article.

Payers and Alternative Payment Models (APMs) are turning to palliative care programs as a way to offer value-based end-of-life care.

Increasing hospice services can reduce hospital admissions among all residents of a nursing home, including those not enrolled in hospice.

Why do providers continue to enter into business/referral relationships without meeting applicable requirements, thereby violating the law?

One of five people with self-care disabilities reported negative consequences from not having help with activities they had trouble performing on their own.

Fall-related injuries are a major reason why seniors are readmitted to the hospital within a month after being discharged, a new study finds.

A panel of eldercare experts released its definition for person-centered care, which stresses collaboration between the patient, family, and provider.

A recent study in the New England Journal of Medicine by Partners HealthCare System examines community-based linkages to population health.

Medicaid’s reform will lead to greater care coordination, a focus on reducing costs and more possibilities of risk and preferred provider networks.

A report from MedPAC staff outlined the pros and cons of an episode-based payment approach compared to a stay-based payment approach.

Congressional approval of the IMPACT Act in October 2014, mandates the development and implementation of a standardized post-acute care assessment, too.

Exploring similarities in PAC settings flushes out what is presently aligned for the model to work, and identifies where there are gaps.

SUBSCRIBER CONTENT Key strategies to accomplish clinical continuum includes reducing the cost of care and developing post-acute tools for redefining partnerships.

SUBSCRIBER CONTENT Novant participated in a VHA research project that significantly reduced overall readmissions and those related to adverse drug events.

SUBSCRIBER CONTENT From July to December 2014, VNA Healthtrends, a leading home health provider, enrolled 51 patients in their Hospital to Home Program.

SUBSCRIBER CONTENT Patients sent home after knee and hip replacements do not have higher rates of medical complications, returns to the hospital or E.R. visits

SUBSCRIBER CONTENT Palliative care focuses on relieving patients’ stress, pain and other symptoms as their health declines, and it helps them maintain their quality of life.

SUBSCRIBER CONTENT Aetna’s Compassionate Care Program is designed to improve the quality of patient care for individuals with life-threatening illnesses.

In a large cohort study, hospice visits in the last 2 days of life by professional staff varied by race, hospice program, and geographic region.

Despite recommendations to the contrary, only about half of elderly patients with advanced cancer receive palliative care.

A new guidance statement to define high-quality primary palliative care delivery in medical oncology has been developed by ASCO and AAHPM.

Spending on Medicare beneficiaries in their last year of life accounts for about 25% of total Medicare spending on beneficiaries age 65 or older.

Four key trends in hospice care are contributing to a paradigm shift and impacting the future of Medicare hospice providers and other providers.

Highmark offers unique palliative care services to its Medicare Advantage members and supports hospital palliative care through value-based contracts.

The ACO Investment Model encourages new ACOs to form in rural areas and Medicare Shared Savings Program ACOs to take greater financial risk.

17 states are implementing accountable care strategies in Medicaid or state employee health programs and patterns have begun to emerge.

The ACO model has the right incentives to reduce variation, spur innovation, and improve quality in end-of-life (EOL) care

Early evidence suggests that, under episode-based incentives, clinicians and organizations can improve the value of care for certain episodes.

SUBSCRIBER CONTENT A home-based palliative care program tested within an ACO showed cost savings and reduced hospital admissions for patients near the end of life.

The ACO Medicare-Medicaid Model is focused on improving quality of care, improved care coordination, and reducing costs for Medicare-Medicaid enrollees.

A study by Dartmouth Institute For Policy and Clinical Practice finds coordinated care for patients with complex needs a big winner for ACOs.

A study in The American Journal of Accountable Care provides a window into how ACOs manage high-risk, moderate-risk and low-risk patients.

SUBSCRIBER CONTENT Geisinger Health Plan published a study that found a telemonitoring intervention for heart-failure patients led to reductions in readmissions and cost.

SUBSCRIBER CONTENT The use of health coaches supported by the tablet-based software significantly reduced readmission rates among at-risk Medicare patients.

CMS is shaping a framework intended to allow better comparisons of post-acute care provided in four different healthcare settings.

Greater use of Medicare Advantage over traditional fee-for-service Medicare has been associated with fewer overall hospitalizations.

In 2015, the proportion of hospitals receiving a penalty increased to 78% – up from 64% and 66% in 2013 and 2014, respectively.

The IMPACT Act will require hospitals, rehab facilities, and home health agencies to develop a discharge plan based on the goals of each patient.

Patient "activation scores" can identify those who might benefit from making behavioral changes, helping improve outcomes and prevent unnecessary costs.

Patients 65 and older who have ambulatory surgery are much more likely to be readmitted to the hospital within 30 days than younger patients.

Significant studies are questioning whether a 30-day interval for readmissions is the best measurement for Medicare-related penalties.

Data on 2,000 patients showed telephone follow-up for older adults following discharge from the emergency department did not affect readmission rates.

SUBSCRIBER CONTENT FirstHealth of the Carolinas has developed an innovative care delivery model to effectively manage high-risk patients with chronic disease.

SUBSCRIBER CONTENT MedPAC has had recent discussions on current discharge planning procedures, resulting in possible changes in the ways patients are discharged.

Older adults are at increased risk for adverse events after surgical procedures. Loss of independence is an important patient-centered outcome measure.

30-day readmission rates are widely used to measure hospital penalties. Yet, many question if this is the correct interval by condition.

Telehealth policy develops much more slowly than the rapidly advancing technology, but incremental changes are taking place.

Medicare spending for home healthcare more than doubled between 2001 and 2017, accounting for $17.7 billion spent on home health services.

Approximately four million adults in the United States are home bound, and many of them cannot access office-based primary care.

In 2014, 14% of inpatient stays were readmitted within 30 days. More than one-third of these readmissions occurred within seven days.

This issue of FutureFocus highlights the innovation of an in-home, physician-led model working collaboratively with a payer to manage complex care.

In this issue of FutureFocus, we offer up 10 ways to identify future partnerships between physicians and the home care industry.

This issue of FutureFocus identifies the highest risk of readmissions that are impacting outcomes in the CMS value-based purchasing program.

The new Primary Cares Initiative that will transform care and payment for complex, high-need patients who are able to stay healthy in their own homes.

Studies show that patients sent home after knee and hip replacements do not have higher rates of complications than those who went to rehab facilities.

As the Baby Boomer generation ages and the elderly population grows, the demand for the services of home health aides and personal care aides will continue to increase.

New guidance has been issued by CMS about where Medicaid beneficiaries can receive home and community-based services, impacting many providers.

A new RFI has been issued by CMS to ask for stakeholder feedback about the best ways to incent EHR adoption in post-acute settings.

The OIG posted Advisory Opinion No. 10-03 on March 6, 2019, which permits hospitals to provide free, in-home follow up care to discharged patients.

Monitoring the health of your organization supported by real-time key performance indicator data can help to de-risk the future of your organization.
We want you to think boldly about your future! Unlocking growth and business development opportunities for your organization requires a deep understanding of industry trends, evaluating different growth drivers based on healthcare and home care market transformations, comprehending the strategic direction of your referral sources, and uncovering your direct path to growth.
With three decades of unwavering commitment, we take pride in our proven track record as vital educators and growth strategists within the home care industry and its ecosystem partnerships. Our comprehensive suite of education and consulting services drives innovation for navigating ongoing disruptions, capitalizing on emerging growth opportunities, and creating a bold new future.
Just complete and submit the form, and a member of our team will be in touch shortly.
Just complete and submit the form, and a member of our team will be in touch shortly.
Just complete and submit the form, and a member of our team will be in touch shortly to discuss membership fees and additional details.
Just complete and submit the form, and a member of our team will be in touch shortly to discuss membership fees and additional details.
Just complete and submit the form, and a member of our team will be in touch shortly to discuss our various strategic initiatives.

30262 Crown Valley Parkway
Suite B 407
Laguna Niguel, CA 92677
remington@remingtonreport.com
Copyright © 2012 – | The Remington Report | All Rights Reserved | Privacy Policy | Terms & Conditions | Powered by LeadWorks

Click on any title to read the article.

Click on any title to read the article.

Click on any title to read the article.

Click on any title to read the article.

Click on any title to read the article.

Click on any title to read the article.

If you are not receiving our newsletters, then the first thing to do is to check your spam folder. If you can see our newsletters there, then you should whitelist them/report them as not spam. The process for doing so is typically documented by your email product. You can also add us to your contact list (remington@remingtonreport.com).
If you can’t see our newsletters anywhere in your spam folder, then most likely they were filtered out by your organization’s firewall. In this case, you should ask the security team of your IT department to whitelist incoming mail originating from the following IPs:
| CIDR | Start of Range | End of Range |
|---|---|---|
| 173.236.20.0/24 | 173.236.20.2 | 173.236.20.254 |
| 192.92.97.0/24 | 192.92.97.2 | 192.92.97.254 |
| 52.128.40.0/21 | 52.128.40.0 | 52.128.47.255 |
You should also ask them to whitelist the domain: remingtonreport.com
Forgot your password? Just click the "Forgot Password?" link below and enter the subscriber's username or email address. An email will be sent to you with a password reset link. Be sure to check your spam and/or junk mail folders for the email.